

Yvonne, a community health worker/RECO in the DRC, walks through her neighborhood and visits homes, amplifying important health messages and helping her community access health services.
To promote the adoption of behaviors that advance health and well-being, IMA World Health (IMA) implements high quality social and behavior change (SBC) strategies both as stand-alone interventions and, most frequently, as part of integrated methodologies across our programming. IMA’s approach to SBC is inclusive, human-centered and highly participatory. We work at the community and district level to co-design and co-create activities based on joint needs assessments. By leveraging community expertise, IMA champions local stakeholders and implements programming that considers the cultural and social norms and environmental determinants of diverse contexts.
Our proactive approach
IMA takes a proactive approach to SBC in our health programming, intentionally planning for shocks and stressors in fragile settings. Our approach follows five principles:
- Use two-way participatory approaches to increase accountability and health care-seeking behavior;
- Map opportunities in SBC linked to the resilience capacities;
- Prepare community health workers prior to crises to support individuals, communities, and households during shocks and stresses;
- Identify coordination and collaboration structures; and
- Be nimble and pivot as needed.
Through this approach, IMA helps establish partnerships and more effective risk communication and community engagement (RCCE) efforts between health service providers and the people they serve. Coordinating partners and activities in advance of crises as part of this approach also allows for improved response and mitigation measures to be enacted. By being proactive, IMA ensures our SBC activities are strategically interwoven throughout the humanitarian-development nexus.

Josue Nsibiro, a facilitator of men's engagement in the US government funded Tushinde project, hosts sessions with men to improve attitudes about women in Goma, DRC.
Social accountability
Social accountability and community engagement are essential for building trust and capacity in a health system. However, incorrect information, stigma or socio-economic barriers can prevent both from meaningfully taking place. To overcome these challenges, IMA utilizes SBC activities, such as community scorecards and community health committees, to increase community participation and the two-way flow of information in health service delivery.
Accompaniment
At IMA, we understand that true innovation and transformation can only be achieved by supporting, leveraging and elevating the existing capabilities of the people, communities and organizations closest to where change is needed. This is why we call our approach to local capacity strengthening, accompaniment. For us, accompaniment is an intentional, collaborative and respectful process where we support mutual effectiveness, learning and resilience. At the core of our accompaniment model lies the A-CORD framework: To Assess - Commit, Organize, Relate and Deliver. This framework facilitates a participatory process for local organizations to self-analyze their strengths and challenges, supports their comprehensive action planning, and promotes continual collaboration, adaptation and learning.
WSR: "Whole System in a Room"
IMA ensures that our SBC interventions focus on the target population, considering their specific contexts and the multitude of stakeholders, to understand and address the core issues effectively. Starting from the needs assessment phase through project design, implementation, and monitoring, IMA brings all of the system’s actors into the fold to routinely garner their important contributions and ensure their ultimate buy-in and ownership.
Complexity-aware M&E for adaptive management
In addition to rigorously collecting and analyzing quantitative data, IMA employs complexity-aware qualitative M&E approaches to help us better understand important nuances and afford project participants, especially women and youth, more freedom to tell their stories—ultimately informing adaptive management and improved outcomes. Some examples of such methods include Photovoice, Most Significant Change (MSC), and digital diaries. We also use vignettes, brief stories about fictitious people who are very similar to the target population, to solicit people’s views on social and cultural norms and their personal experiences with related situations. In being able to comment freely about someone else’s story rather than their own, the potential influence of stigma and other social pressures is reduced, resulting in more people sharing their truths. Additionally, IMA uses project Knowledge, Attitudes, and Practice (KAP) surveys, Likert scales and card pile sorting exercises, which help staff course-correct to improve project outcomes.

Project participants in Uganda utilize Photovoice to identify constraints women face regarding food security, income, and decision-making at the cooperative and household levels.
Championing SBC in Tanzania
Our programming in Tanzania serves as an important case study for implementing SBC initiatives. IMA spearheaded the ASTUTE program, which effectively employed behavior change communication to improve nutrition outcomes and specifically combat child undernutrition. As part of the USAID-funded MOMENTUM Integrated Health Resilience, IMA applies SBC strategies in Tanzania to enhance access to health services and empower communities to manage natural resources sustainably, thereby improving their livelihoods and conserving biodiversity. Through the Public Sector Systems Strengthening Plus (PS3+) project, IMA collaborated with the Tanzanian government to institutionalize public sector systems that effectively respond to citizens' needs for essential, high-quality public services, especially for underserved populations. Additionally, IMA has incorporated SBC methodologies into our initiatives to combat neglected tropical diseases (NTDs) in Tanzania, while also strengthening the health system.

Nurse Praxeda Kahwa measures the mid-upper arm circumference of a child at the Nyamagana District Hospital in Mwanza, Tanzania through the ASTUTE program, led by IMA World Health.
IMA convenes an SBC community of practice across our fellow Corus organizations, including staff from health, nutrition, agricultural livelihoods development, technology, and community development sectors.
To learn more about our SBC work and the community of practice, contact:
Dr. Kamden Hoffman, Technical Director, Social & Behavior Change
PROJECT HIGHLIGHTS
MOMENTUM Integrated Health Resilience
IMA World Health leads the five-year, USAID-funded MOMENTUM Integrated Health Resilience program, which is part of a suite of innovative MOMENTUM awards designed to holistically strengthen quality maternal, newborn, and child health in host countries around the world. Working alongside local organizations, governments, and humanitarian and development partners in fragile settings, the project helps accelerate reductions in maternal, newborn, and child illness and death by increasing the capacity of host country institutions—at the national and subnational levels—to strengthen health systems, adapt evidence-based policies, guidelines and practices to their specific contexts, collect and utilize data to inform interventions, and increase partnerships between various public and private stakeholders to disseminate learning, leverage resources and scale efforts to achieve better outcomes. IMA's SBC approach is interwoven throughout the activities with the team producing a roadmap based on their experience and learnings for how to utilize SBC to improve demand for and use of quality health services in fragile settings.
Addressing Stunting in Tanzania Early (ASTUTE)
Through the FCDO-funded ASTUTE program, IMA strengthened the capacity of local government authorities to address child stunting, achieving between 7-12% stunting reduction across five regions of the Lake Zone: Kagera, Kigoma, Mwanza, Geita and Shinyanga. The project trained nearly 7,800 district health workers and non-health sector service providers and reached 17.6 million nationally through mass media campaign. Additionally, 6.4 million mothers, caregivers and decision-makers benefited with improved child-feeding information through home visits conducted by 6,000 community health workers. As part of the project, IMA created a toolkit to provide government and local organizations with programming recommendations and tools to help implement successful multisectoral SBC interventions aimed at preventing and reducing stunting.
Sesame Marketing and Exports (SESAME)
As a part of the Corus International family of organizations, IMA assisted our fellow Corus organization Lutheran World Relief with SBC activities for their USDA Food for Progress SESAME Project during the COVID-19 pandemic. The goal of the overall project was to increase the quality and volume of sesame exports through improved agricultural practices and market systems strengthening in the regions of Boucle du Mouhoun, Est, Cascade and Hauts Bassins in Burkina Faso. Through the project’s existing agricultural extension online platform, IMA and LWR provided up-to-date information about pandemic-related impacts on agriculture and provided more than 5,000 farmers with information to protect their health and livelihoods. The platform not only provided standard COVID information but gave farmers specific information such as locations and times in their districts or regions where they could sell produce or purchase inputs while limiting exposure to COVID.
Tushinde Ujeuri
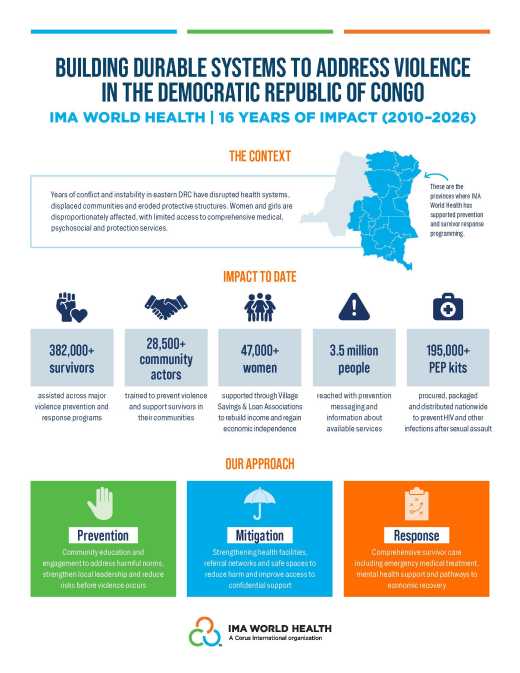
Funded by USAID, the Tushinde Ujeuri project supported communities in eastern DRC to prevent and respond to violence against women and girls with the goal of reducing violence, combating stigma and improving holistic care for survivors. Building on the highly successful USAID-funded Ushindi program implemented by IMA (2010-2017), the Tushinde project provided urgent medical care, psychosocial counseling, legal support, and socioeconomic support (access to village savings and loan associations, literacy circles, and women’s groups) to help survivors gain financial independence and social support. To create change at the community level, the project’s SBC strategy used a peer group approach and engaged local leaders, working largely through schools. IMA helped establish 194 youth clubs to educate adolescents (ages 10-19). Using an evidence-based curriculum tailored to the DRC context, the clubs offered specific information to increase protection for women and girls. These youth clubs covered topics such as the impact of violence against women and girls on families and the community and the risks of early marriage. Similarly, in Ushindi, IMA supported the formation of over 400 “noyaux communautaires,” or Community Core Groups, involving 20-30 voluntary local leaders, faith leaders, and village chiefs in educating their communities and promoting discussions on violence against women and positive masculinity.
Afya Jijini
Afya Jijini, which translates to “health in the city,” was a three-year USAID contract (with two option years) with the strategic goal of improving Nairobi City County’s (NCC) institutional and management capacity to deliver health services. The program improved access to and use of maternal, neonatal and child health services; water, sanitation and hygiene (WASH); and nutrition services. The program also helped the government roll out newly revised Integrated Management of Childhood Illness (IMCI) guidelines and improve the coverage and reporting on childhood immunization in Nairobi County. When the COVID-19 pandemic hit Kenya, the project provided technical assistance to the Nairobi Metropolitan Services (NMS) to develop its RCCE strategy and interventions. The project tapped a cohort of 500 previously trained and trusted Community Health Volunteers (CHVs) to serve as the frontline for COVID-19 SBC messaging and contact tracing efforts. These volunteers, who had been engaged previously for MNCH and HIV messaging, pivoted to provide evidence-based messaging on COVID-19 prevention at the individual, household, and community level; how to cope with the pandemic and lockdowns; and allaying common fears, such as the widespread belief that patients often contracted COVID-19 by visiting health facilities. CHVs were also trained to conduct contact tracing and support home-based isolation and care for clients who could safely be managed at home rather than in isolation centers. Project coaching focused on improving rapport with clients to help identify infected patients who may be afraid to share their information as well as helping households understand when patients may require facility-based care.
Access to Primary Health Care (ASSP) and Access to Health Systems Support (ASSR)
During eight years of implementation, ASSP and its follow-on project ASSR improved the health of women, adolescents and children through support for disease prevention, delivery of health care and health systems strengthening. With funding from the UK’s Foreign, Commonwealth & Development Office (FCDO), the projects supported an estimated 9.7 million people across 52 health zones in five provinces, strengthening the health system by focusing on priority interventions such as the treatment of malaria, pneumonia and diarrhea; nutrition; obstetric and neonatal care; family planning; immunization; and water, sanitation and hygiene (WASH). IMA introduced effective people-centered best practices to ensure community engagement in the continuity of quality primary health care, such as community scorecards and community health committees. These activities fostered social accountability, the two-way flow of information and trust between communities and the health system. The health facilities utilizing scorecards found they helped improve the consideration of women's needs in community health committees, led to better coordination of health and nutrition services, and resulted in increased immunization rates as well as decreased malnutrition rates and malaria cases.
Technical Resources
-

Technical Approaches
Local Capacity Strengthening Technical Overview
-
Emergency Situation Reports
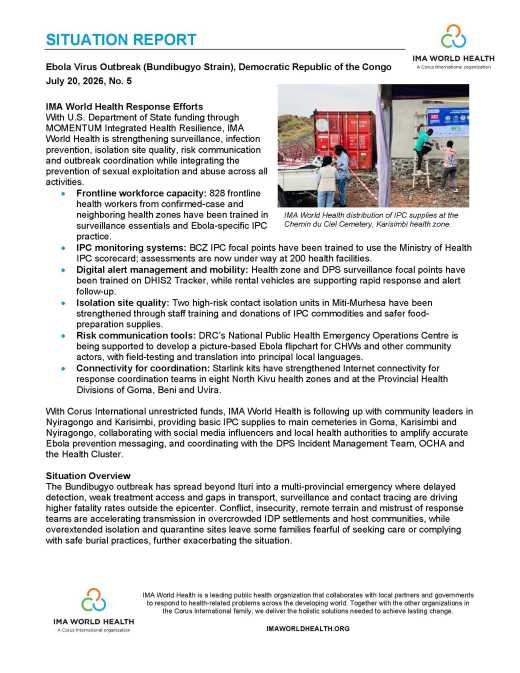
Situation Report #5: Ebola Outbreak in Eastern Democratic Republic of the Congo
-
Technical Approaches
Promoting High-Impact Health Practices
-
Emergency Situation Reports
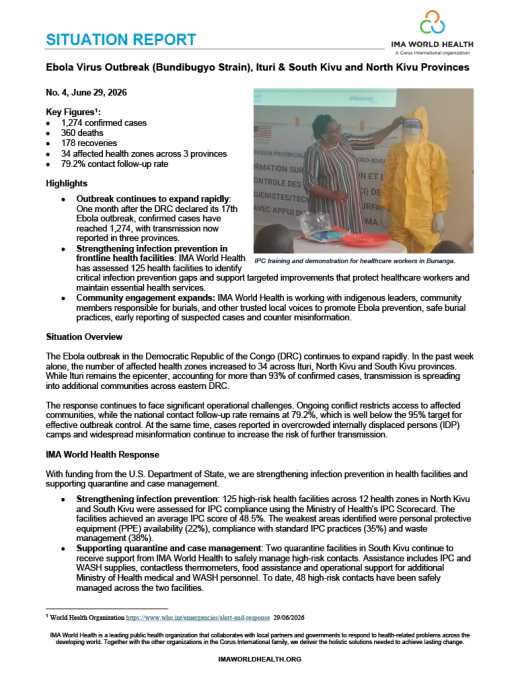
Situation Report #4: Ebola Outbreak in Eastern Democratic Republic of the Congo
-
Emergency Situation Reports
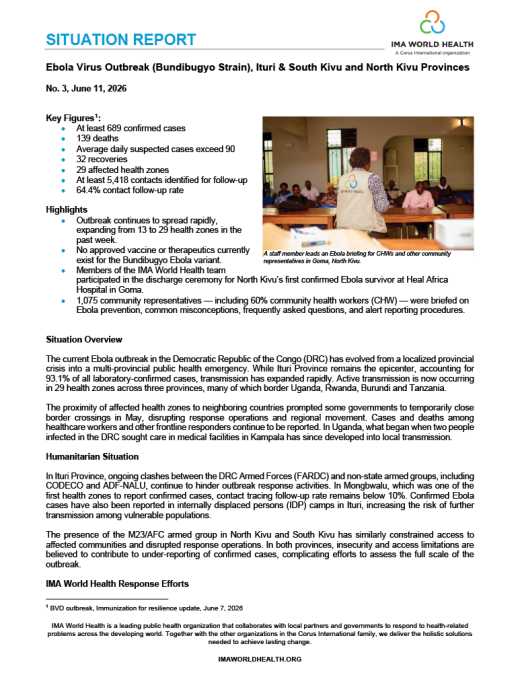
Situation Report #3: Ebola Virus Outbreak
-
Reports
16 Years of Impact: Addressing Violence in the DRC
-
Technical Approaches
Mpox Emergency Response Technical Overview