



Struggling with data management in low-resource settings hampers effective health care delivery. DHIS2, an open-source, flexible, and scalable digital platform, is revolutionizing this landscape. It streamlines data collection, enables real-time or near-real-time reporting, and eliminates delays caused by outdated, paper-based systems. With its offline functionality, health workers in remote areas can capture and store critical data, syncing it when connectivity allows. By providing timely, accurate insights, DHIS2 empowers evidence-based decision-making, strengthens health care systems, and drives better outcomes where they are needed most.
A trailblazer in digital health transformation
IMA World Health has been at the forefront of revolutionizing health data systems since 2006. Initially, the Government of DRC's transition from GESIS, a paper-based platform fraught with inefficiencies and restrictive features, underscored the critical need for a more adaptable solution. Rising to the challenge, IMA World Health introduced the District Health Information System (DHIS) 1.4 in South Kivu's 28 health zones in 2009, customizing it to local needs and streamlining data collection, processing, and quality. Building on this success, DHIS2 was rolled out in 2015 across all 52 health zones under IMA’s leadership. This massive undertaking included connecting health centers nationwide to the internet, equipping health zone offices with essential technology, and training thousands of health care workers to manage and report data effectively. Today, DHIS2 is routine in the delivery of quality health care across DRC.
Learn more about how IMA World Health helped pave the path to digitized routine data.
Strengthening health systems through DHIS2
Since 2016, IMA World Health has used DHIS2 as a strategy to strengthen national health systems. In both program implementation areas and nationally through advocacy and partnerships, IMA World Health leverages DHIS2 to contribute to the global public health dialogue and advance development goals.
IMA World Health enhances program performance and impact by leveraging the DHIS2 platform for improved data capture and analysis. Simultaneously, we strengthen the DHIS2 capabilities of local counterparts and governments, promoting accountability and fostering adaptive management practices. This includes ensuring up-to-date, reliable systems are in place to support three separate yet integrated processes: (1) primary data collection, (2) data storage of multi-source data, and (3) analytics for reporting, data usage and presentation.
Project Highlights
Access to Primary Health Care (ASSP)
With funding from the UK’s Foreign, Commonwealth & Development Office (FCDO), the IMA-led ASSP played an instrumental role in introducing and scaling up DHIS2, a goal which seemed beyond reach to most national stakeholders at the outset of the project given geographic barriers, technological limitations at the time. ASSP and its subsequent follow-on project, ASSR, used a health system strengthening approach that emphasized use of quality data to improve planning, management, and health outcomes. ASSP helped the Congolese government increase the use of its national health information system (SNIS) and address facility level gaps, such as equipment, training, and health zone-level capacity.
Today, more than 90% of health facilities in all 52 ASSP health zones submit regular, accurate, and transparent DHIS2 data. On average, over 1,600 health facilities submit reports each month. The Ministry of Health provides monthly feedback using this data to Provincial Health Information Officers who have been trained by IMA to use data for adaptive management, dialogue, and decision making. This includes user-friendly dashboards with analysis of each program area: service utilization, reproductive health, and vaccination. IMA also provides technical assistance to the Ministry of Health in delivering training to health care workers in the rest of the country.
ASSP provided extensive technical assistance to the Ministry of Health’s Directorate of the National Health Information System (DSNIS) within a consortium of donors including the Global Fund and the World Bank. IMA seconded a Senior Technical Advisor to lead multi-partner HMIS strengthening efforts and provided expertise in identifying data and information needs to be addressed by DHIS2, technical assistance for development of national health information policies, ongoing software configurations and updates, and review of primary health care indicators, data collection forms, training materials, and supervision checklists. IMA improved data collection tools to be more concise and incorporate indicators from vertical programs, such as the national vaccination and malaria efforts, to reduce parallel reporting systems. ASSP built software and data management skills that connected country programs to HQ staff through training in Washington DC, Indonesia, Kenya, Haiti, and Tanzania and built the capacity of targeted Provincial Health Division (DPS) offices, health zones (HZs), and health centers (HCs) to utilize DHIS2 data for program planning and implementation. Overall, ASSP trained more than 500 people in 52 health zones in DHIS2.
ASSP established a HQ-based cloud data system (ADVISE) to comply with more sophisticated technological capacity and data handling requirements. Centralized data access also increased accountability, transparency, and better reporting. To support use of the data in peer-reviewed research, a Research and Writing Working Group in partnership with Brigham Young University, the Ministry of Health, and ASSP staff to collect, analyze, interpret, and present program data was established.
ASSP infrastructure investments to support DHIS2 roll out included installing VSAT (Very Small Aperture Terminal)-linked systems and satellite dishes that transmit data to and from 52 health zones in Congo. Other support tracks daily internet availability in each of the ASSP zones helping monitor health facilities’ ability to submit timely, accurate and transparent data using DHIS2, establish baseline internet access for any future projects and plan VSAT installation and maintenance with provincial technicians.
In times of crisis, such as the Ebola outbreak and COVID-19 pandemic, the Ministry of Health was positioned to use DHIS2 for critical surveillance and data management support. During the Ebola outbreak, this included establishing an electronic database to capture patient and contact data and creating data dashboards and other tools to support on-going monitoring of the outbreak.
Rapid Results Health Project (RRHP)
As part of a five-year flagship health initiative supported by South Sudan's Ministry of Health and the World Bank, IMA World Health spearheaded efforts to strengthen the capacity of the Upper Nile and Jonglei State Ministries of Health, along with 24 County Health Departments. This included facilitating the successful rollout of DHIS2, enhancing the efficiency and effectiveness of health data management systems. This resulted in the effective roll out of a Basic Package of Health Services.
At the national and state levels, RRHP developed the Ministry of Health’s Health Information Systems Program (HISP) team capacity, including co-development of DHIS2 1.4 software and conducting trainings for ministry staff on how to set up DHIS2 and troubleshoot it. IMA, CHD and State/National Ministry of Health conducted joint monitoring on a regular basis (every 2-3 months) using quantify supervisory checklist (QSC) to ensure data quality. As capacity increased, IMA organized advanced DHIS2 trainings in Data Quality and use of Data for Action.
At the state and county levels, RRHP trained County Health Department (CHD) staff in leadership and management, advancing local ownership of the Basic Package of Health Services approach. M&E officers were trained on DHIS2 (from basic to advanced level) to ensure quality data reporting and utilization of the data in decision making at facility and CHD level. DHIS2 software enables the county staff to enter and export health facility data which can easily be imported by the Data Manager and incorporated into the database system.
RRHP also made significant investments in Information Technology (IT) infrastructure, including installation of solar powered VSAT satellite internet in 22 out of 24 counties that enabled continuous and timely reporting through DHIS2 from CHDs from remote counties where other means of communication is practically impossible.
Additionally, IMA’s Corus International counterpart, Charlie Goldsmith Associates Technologies (CGAT), has built inter-operable systems which compile various health datasets under the publicly available platform: https://www.southsudanhealth.info. These research tools draw heavily from DHIS2.
Afya Jijini
IMA World Health worked with Kenya county and sub-county governments to improve health governance, accountability, policy development and implementation. The USAID-funded Afya Jijini project designed and implemented health interventions and approaches, including HMIS with DHIS2, that could be taken over within a finite time by county governments and local communities. Afya Jijini collaborated closely with Nairobi City County (NCC) counterparts to develop and implement a County M&E Framework and strengthen existing M&E systems. By the end of the project, all M&E capacity building and data collection efforts, from planning to execution, were led by the NCC drawing on project technical support as needed.
The project also improved integration of WASH into Kenya’s HMIS, improving WASH data collection, analysis, and use. Specific WASH DHIS2 training and reporting tool components were developed, complementing IMA’s mentorship to subcounty WASH focal persons, Health Record Information Officers, and community health assistants. As a result, WASH-related data and reporting has increased within DHIS2 from as low as 8% to 75% currently and the online UCLTS portal.
The NCC now supports sub-county teams in not only routine health data collection, but also quarterly review meetings to identify and address performance challenges. Combined with capacity strengthening, these meetings showed how data can be used to improve performance and improved reporting rates. The program institutionalized data quality assessments (DQAs) and use of data at facility, sub-county and county levels so that healthcare workers could identify their results and learn how to address data gaps at point of source to avoid entry of errors into the DHIS2 platform.
At the health facility and sub-county level, DHIS2 data is used to improve the tracking and forecasting of essential commodities to improve the timeliness of delivery and distribution. Nairobi County trained 120 healthcare workers in reporting on anti-retroviral therapy (ART) commodities in DHIS2 and 120 county and sub-county pharmacy personnel on how to input data into DHIS2 and undertake commodity data analysis. To improve commodity management, Afya Jijini also trained 50 healthcare workers at clinical point of care on IQ Care or Web ADT linked to DHIS2. Better commodity documentation and reporting into the DHIS2 platform has also improved better prescription practices and maintenance of reasonable stock status. Consequently, a 95% monthly reporting rate for HIV and family planning commodity reporting on the Health Commodity Management Platform and DHIS2 was recorded.
For further scale up, IMA partnered with the NCC and Palladium to introduce electronic medical records and point-of-care reporting for HIV clients at 29 high-volume facilities. Lessons learned by the NCC has further triggered the county to consider introducing similar data management systems in health systems management for both HIV/AIDS and family planning. At the community level, RRHP worked with the County government to train community health volunteers on standard reporting tools, enabling the entry of some of the first community-level data into DHIS2.
Sierra Leone Interlinked Health Registry
CGAT, with funding from DFID through the CHANGES consortium, conducted a feasibility study and provided recommendations on creating an Interlinked Health Registry - essentially a health sector MIS consolidating health data in one place for comparative and planning purposes.
Technical Resources
-

Technical Approaches
Local Capacity Strengthening Technical Overview
-
Emergency Situation Reports
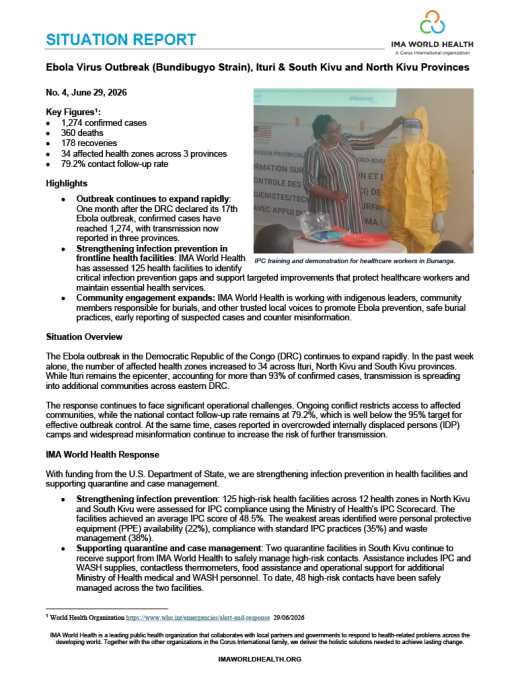
Situation Report #4: Ebola Outbreak in Eastern Democratic Republic of the Congo
-
Reports
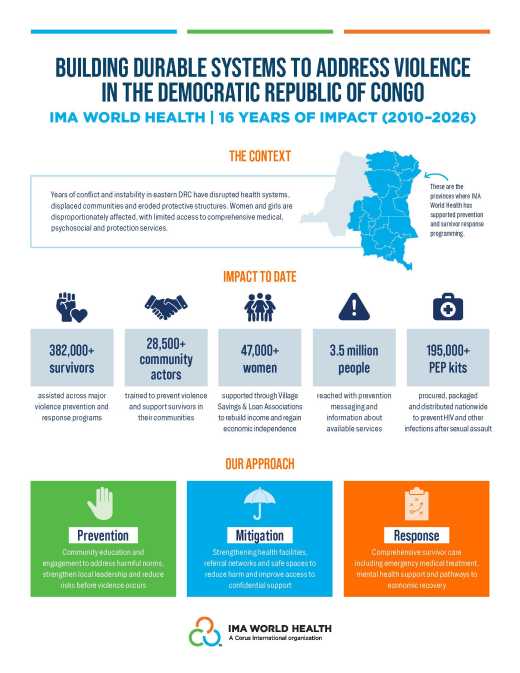
16 Years of Impact: Addressing Violence in the DRC
-
Technical Approaches
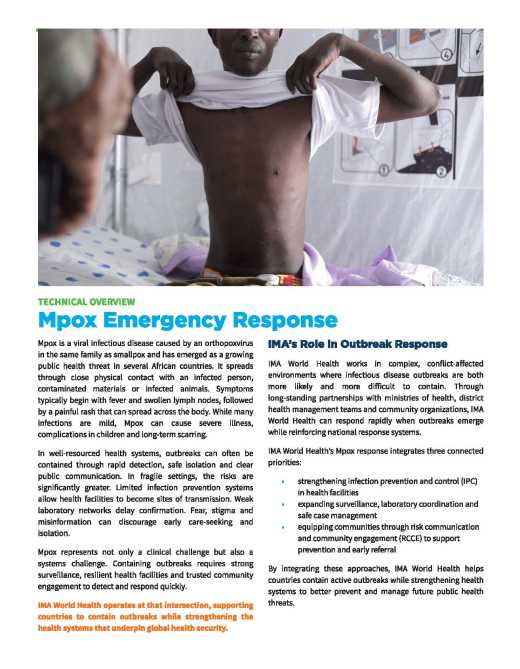
Mpox Emergency Response Technical Overview
-
Project Overviews
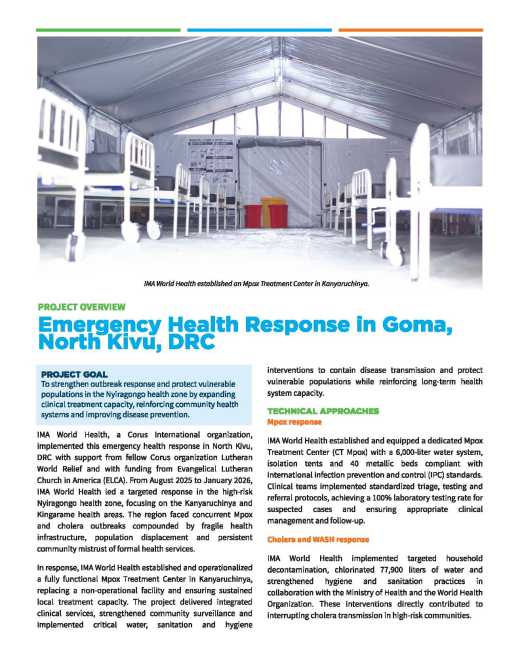
Emergency Health Response in Goma, North Kivu (DRC)
-
Case Studies
Last Mile Health Care: How Faith-Based Workers and Mobile Clinics are Bringing Health, Healing, and ...
-
Case Studies
Community Health Workers in Faith-Based Health Systems: First, Last, and Enduring Responders to Huma...

